
What is scoliosis?
Scoliosis is a disease characterized by abnormal side curvature of the spine. In scoliosis, the external appearance of the spine looks like an S or C letter. The disease usually develops in pre-adolescence and adolescence. Scoliosis can occur alone or together with kyphosis (forward hump).
What are the causes of scoliosis?
Scoliosis is not a single disease and has many causes. The most common type is idiopathic scoliosis, which usually occurs during adolescence and is more common in girls. Although the cause is not known exactly (thus called idiopathic), genetic factors are believed to play an important role in this disease.
Congenital scoliosis is caused by developmental anomalies in the spine during embryological development. In these cases, scoliosis is already present by the time when the baby is born. However, in the vast majority of these cases, scoliosis goes unnoticed in the first months, and the curvature progresses as the baby grows up. When the curvature reaches a particular degree, parents notice the disease and seek medical advice.
Scoliosis can also develop due to weakening of the muscles that support the spine. For instance, scoliosis that develops in patients with genetic diseases of the muscles and nervous system, as well as with cerebral palsy, belongs to this category.
Scoliosis can develop not only in children but also in adults and elderly people. For example, it is common to find long-term lumbar stenosis, disc herniation, and disc degeneration. This type of scoliosis usually develops in the lumbar region and does not lead to significant angulation.
Spinal injuries, tumors, and other diseases, such as fluid accumulation in the spinal cord (syringomyelia), can also cause scoliosis.
What are the symptoms of scoliosis?
Generally, the chief complaint of scoliosis patients’ is the visible deformity of the spine. This deformity is usually noticed by the patient or the parents. In typical cases, the curvature develops in the back (thoracic) area. It is also common for the lower back (lumbar) region to be affected.
The neck (cervical) area is generally spared. Usually, there is also the rotation of the spine around its own axis (rotation) in addition to sideway angulation. In these cases, the rib cage is bulged on one side and flattened on the opposite side. Some of the common symptoms of scoliosis are listed below:

- Obvious spinal curvature when looking at the spine from behind
- Pronounced asymmetry when the patient leans forward
- Differences in hip and shoulder heights
- Different distances from the body to the arms
- Asymmetrical chest
- Posterior rise in one of the shoulder blades
- One leg is longer than the other
- Back and/or low back pain
- Shortness of breath, weakness, easy fatigue
- Unfitting clothes to the body
- Increased pressure on the nerves due to scoliosis can cause leg pain, fatigue, and spasms in the back and waist muscles. If the rib cage is deformed due to scoliosis, heart and respiratory problems are also encountered.
How is scoliosis diagnosed?
Physical examination is usually sufficient for establishing the diagnosis of scoliosis since the deformity is apparent when the patients are standing. During the examination, the patient should lean forward to visualize the deformity better. Meanwhile, the angle measuring device placed on the back gives an estimate of the curvature’s degree.
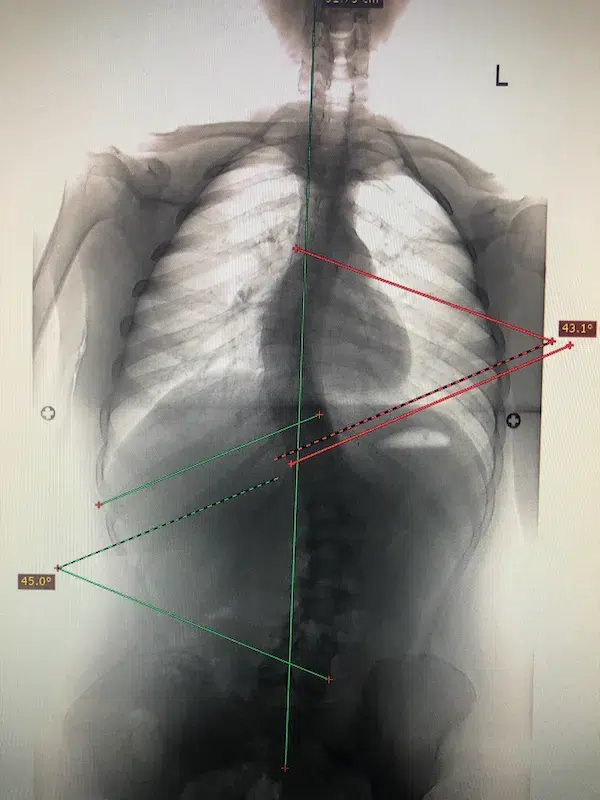
Imaging methods play a great role in the diagnosis of scoliosis. X-ray is the most commonly used utility because it shows the thoracic and lumbar segments on the same image. The degree of scoliosis is evaluated by measuring the angle of the curvature. This angle is known as the Cobb angle and is measured on anteroposterior X-ray.
Lateral flexion X-rays should also be obtained in order to evaluate spine flexibility. These images provide important information for the optimal treatment.
Magnetic resonance imaging (MRI) provides very important information about the soft tissue and the spinal cord itself. Computed tomography (CT) is used only in high-grade, complex cases. Nowadays, it is possible to obtain excellent 3-dimensional (3D) images with this imaging modality. It provides exceptional visualization of the vertebrae (spinal bones), the relations between them, the presence of the rib cage deformity, and the degree of curvature and rotation. However, since it predisposes the patient to high radiation dose, it is recommended only in cases with complex, high Cobb angle cases.
How is scoliosis treated?

The treatment is tailored individually by considering the age of the patients, the degree and location of the curvature, the physical examination findings, the imaging data, and the progression of the disease over time. Early diagnosis greatly increases the treatment success rate. Management choices include observation, orthosis wearing, physical therapy with muscle training, and surgical intervention. The first option of treatment, observation, is generally applied for curvatures below 20 degrees. More severe cases are managed with physical therapy and active training. Advanced cases require surgical correction.
What happens if scoliosis is not treated?
As with other diseases, untreated scoliosis can present various additional health problems. Especially in cases with progressively increasing curvature, the thoracic cavity becomes compromised, and the patients experience breathing difficulties. Appropriate and early treatment is essential for the prevention of shortness of breath in developing children. However, if the scoliosis is mild and does not cause additional issues, treatment is not required. Patients may be followed with regular check-ups for the curvature progression control.
Physical therapy in scoliosis
It is generally applied in cases with a low degree of Cobb angle. Nowadays, cases up to about 40 degrees can be treated with various physical therapy and exercise methods. Estimating spine flexibility is crucial in these cases since it is the main factor influencing the treatment outcome. For example, in cases of congenital scoliosis resulting from abnormal spine fusion, flexibility is lost. Thus, physical therapy is of no use in these cases. These cases, as well as high Cobb angle cases, should be treated with surgery.
Scoliosis Surgery
Surgery is performed in patients with advanced scoliotic curvature or therapy-resistant cases. Spine stabilizing operations are generally performed in adults and teenagers in whom spine maturation has been completed. This technique, known as spinal fusion, involves inserting screws into the vertebral bones and then fixing the curvature by connecting metal rods to these screws. In some cases, it may be necessary to cut spontaneously fused abnormal vertebral bones. The fixed spine is immobilized and cannot be extended. Therefore, this method is not suitable for young children who are getting taller. A different technique called “growing rod” is more suitable for young children. In this method, a metal rod, which may be extended by an external magnetic field, is used. As the child grows, the length of the rod is adjusted periodically during follow-up visits.
Another non-fusion technique has been developed relatively recently. It includes the use of specific tethers implanted to the convex side of the scoliotic curve. As the child grows, the tether prevents the growth of the convex side, while the concave side can grow unrestricted. The resultant effect straightens the spine over time.
The recovery process after scoliosis surgery is similar to other spine procedures. Generally, the first week is spent in the hospital, daily activities are resumed within one month, and it is possible to start sports activities in the third month.