What is the lumbar disc herniation?
Lumbar disc herniation is a condition when degenerated nucleus pulpous of intervertebral disc slips into the spinal canal, causing compression of the nerve roots.
What is the structure of the lumbar spine?
The spine
The human spine is the major supporting structure of the human torso. It is composed of vertebral bones and connecting joints. For practical purposes the spine is divided into five parts: cervical, thoracic, lumbar, sacral and coccyx.

The lumbar spine comprises five lumbar vertebrae and joints between them. These joints provide mobility to the spine. Each vertebral bone is connected to its neighbor via three joints – two facet joints in the back and a single intervertebral disk joint in the middle and front. These three joints make spine motion segments or articular triad.

The disc joint is the principal one and carries most of the load. It comprises a gelatinous middle part named nucleus pulposus (or simply nucleus), a strong external fibrous ring, annulus fibrosus, and a cartilaginous end-plate covering the bone’s surfaces. The spinal cord runs through the vertebral canal formed by these vertebrae, connecting the brain to the body. The vertebrae protect the spinal cord as it transmits neural signals throughout the body.
The nucleus
Structure and function
The nucleus contains type II collagen, proteoglycans, and water. It is estimated that water constitutes 70-90% of the disc material in the nucleus. 1 Proteoglycans, particularly aggrecan are essential for maintaining high water content through osmosis. The osmotic pressure inside the healthy disc is very high due to proteoglycans. This pressure drives water into the nucleus, leading to swelling and high mechanical pressure. The unique properties of disc material are crucial for these functions.
Nucleus swelling and high osmotic/mechanical pressure are the main mechanisms for maintaining the intervertebral disc joint’s load-bearing capacity. This is similar to a car tire, where high air pressure is essential for driving. In addition to load-bearing, the disc joint is an excellent shock absorber and provides much of the spine’s flexibility. It acts like a spring between vertebral bones.
Metabolism of the nucleus
Disc joints do not have blood vessels. Oxygen and chemicals diffuse passively from neighbor vertebral bones through the cartilaginous end-plate. In other words, vertebral bones feed disc joints. Generally, the nucleus is hypoxic, meaning it has a low oxygen level. Hypoxia is more pronounced in the center due to the distance from the “feeding” bone surface. 2
The primary energy source for the nucleus is glucose, which is metabolized to lactic acid due to an anaerobic environment. The concentration of lactic acid is highest in the center, where the concentration of oxygen is lowest. 2
The faces joints
Facet joints are also very important for normal spine function. Together with the intervertebral disc joint, they constitute the spinal motion segment, a three-joint complex or the articular triad. They are composed of opposing protrusions from adjacent vertebral bones. These protrusions or extensions are called articular processes. Hyaline cartilage covers the contact areas of these bony processes and serves as a gliding surface. Facet joints limit excessive motion vertebral slippage and protect disc joints from overstretching and damage. 3
What is disc degeneration, and how does it lead to a herniated disc in the lumbar spine?
Disc degeneration is a condition characterized by progressive damage to the nucleus pulposus, leading to desiccation, shrinkage, fragmentation, and eventually complete wear-off. It is the principal disease leading to a herniated disc or spinal canal stenosis. Until today, we do not fully understand the cellular and molecular mechanisms that trigger degeneration. It is known that degeneration is linked to aging and mechanical wear.
Under physiological conditions, the normal structure and volume of the nucleus are maintained by a fine balance between the mechanical wear and the ability of cells to restore the losses. However, conditions in the healthy disc joint are quite harsh. Lack of oxygen and nutrients makes it difficult for cells to replenish load-induced wear, especially aggrecan – the main proteoglycan, a type of protein responsible for maintaining disc functions. Loss of proteoglycans and collagen is the main molecular mechanism of disc degeneration. 4
With the loss of aggrecan and other essential proteoglycans, the osmotic pressure in the disc diminishes, leading to disc desiccation. As a result, the mechanical, hydrostatic pressure in the disc diminishes, compromising the load-bearing capacity of the disc joint. Disc height progressively collapses under body weight, leading to spinal stenosis, a condition where the spinal canal narrows, and/or lumbar disc herniation.
Risk factors for lumbar disc degeneration
Overweight, tall people are prone to disc degeneration simply due to higher mechanical load. The same is true for occupational heavy lifting. Children, teenagers, and young adults in their 20s have the highest level of proteoglycans in the disc and do not have disc degeneration unless there is a major predisposing factor.
Availability of nutrients, clearance of waste products like lactic acid, and maintenance of high osmolarity are essential for a healthy nucleus. Disruption of delicate physiological balance leads to disc damage and degeneration. 1 Starting from the age of 30, there is a decline in proteoglycan levels and an increase in waste products, leading to progressive disc degeneration.
Smoking is a risk factor for lumbar disc degeneration 5 The exact mechanism of smoking-induced damage to the disc joint is unknown. Recent research showed that the main factor may be smoking-induced damage to aggrecan via activation of the ADAMTS pathway. ADAMTS is a group of enzymes that degrade aggrecan, a crucial component of the disc joint, leading to degeneration. 6
Degeneration-induced changes in the nucleus and their complications
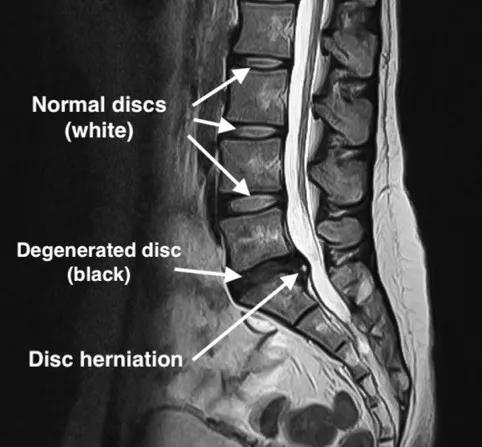
As a result of degeneration, the elastic, viscous, well-hydrated nucleus desiccates, shrinks, wears off, and fragments to pieces. The initial stage of degenerative disc disease is called “black disc disease” due to the loss of water.

High water content is maintained by high osmotic pressure, which is provided by proteoglycans. With the loss of proteoglycans, the osmotic pressure decreases, leading to dehydration, which changes the disc’s MRI appearance from white to black (hence the name “black disc disease”).

Loss of osmotic pressure also reduces intradiscal mechanical pressure and its ability to withstand body weight. Diminishing of elastic recoil force leads to decreased disc height and bulging out of annulus fibrosus.
Also, the loss of nucleus pulposus material causes several changes in vertebral endplates known as Modic changes. Modic changes frequently accompany disc degeneration and show the severity of the disease. As a result of disc degeneration, bone end plates become edematous, eroded, and eventually sclerotic. The progressively shrinking nucleus is fragile and slowly ground between vertebral bone, which acts like millstones. In the later stages, the nucleus pulpous may entirely vanish, leaving empty space. This void space is best visible on a CT scan and is known as the “vacuum sign” or “vacuum phenomenon.”

Pain in lumbar disc degeneration
A degenerated nucleus loses its mechanical properties and cannot withstand body weight. As a result, patients start feeling lower back pain and discomfort. A characteristic feature of this pain is its mechanical nature. Mechanical loading, such as heavy lifting, exercise, or prolonged standing and sitting, increases stress on the spine and can cause pain. Like other joint-related conditions, cold usually triggers the pain. There are several mechanisms contributing to discogenic low back pain.
- A damaged disc is painful due to its inability to withstand normal load and degeneration-induced inflammation. Nerve endings in the discs are responsible for generating and transmitting these nociceptive impulses. Mechanical overloading and the accumulation of lactic acid and inflammatory cytokines irritate nerve endings and cause radicular pain.
- Loss of load-bearing capacity shifts the load to facet joints and other supporting elements. Remember, disc joints and two facet joints make one motion segment. Normally, facet joints take only a small portion (about 16%) of the load. With disc degeneration, facet joints must compensate for diminished load-bearing capacity and carry more load. This extra load induces pain. If facet joints bear too much load for an extended period, they are damaged and become the source of the pain themselves.
- Disc degeneration results in decreased water content in the nucleus pulposus. As a result, high intradiscal pressure diminishes, and the disc joint collapses, leading to instability. Therefore, other secondary supporting structures in and around the spine must step in and restore stability. The spine is surrounded by strong muscles collectively named paravertebral muscles (“para” means nearby). Besides providing motion to the spine, they also act as an “external supporting envelope” and stabilize the spine. These muscles contract to balance unstable segments. Therefore, paravertebral muscle spasm is a usual symptom of degenerative lumbar spine disease. This persistent spasm may become a substantial source of pain.
Lumbar disc herniation
A key feature of disc degeneration is irreversibility. Like many other age-related changes in the human body, the process cannot reverse itself. Currently, there are no effective treatments to reverse disc degeneration. The speed of degeneration may vary, though. Some discs deteriorate fast, while others remain in the initial stages of degeneration for a long time.
As degeneration progresses, the nucleus shrinks more and more and eventually breaks down into fragments. One of these fragments can make a tear in the annulus and slip out. This condition is called a lumbar disc herniation.
As you can see, lumbar disc herniation is not an independent disease, rather it is one possible scenario in the course of disc of degeneration.
Lumbar disc herniation causes other possible conditions and complications. Ruptured disc fragments bulge outward and compress the nearby nerve root(s), a condition known as lumbar radiculopathy. Spinal nerve roots provide innervation to the leg, so symptoms of radiculopathy include pain, numbness or tingling, and weakness in the leg. Severe cases can lead to cauda equina syndrome, a rare but serious condition requiring immediate medical attention.
Cauda Equina Syndrome
In rare cases, disc herniation can cause cauda equina syndrome, leading to severe pain, bladder and bowel dysfunction, and possible permanent damage if not treated promptly. 7 Cauda equina syndrome symptoms may also include significant numbness in the groin area, weakness in the legs, and loss of reflexes.
Types of lumbar disc herniation

There are several types of lumbar disc herniation. Initially, the degenerated nucleus cannot maintain its spring action and maintain normal disc height. As a result, vertebral bones get closer, and the annulus fibrosus bulges out. Later, a piece of degenerated nucleus may slip between annulus fibers and make a local disc protrusion.
A herniated disc may tear the annulus slip under the posterior longitudinal ligament and form an extrusion. At this stage, the herniated fragment has partially or completely lost its connection with the rest of the nucleus. Rarely, slipped fragments may rupture the posterior longitudinal ligament and migrate into the spinal canal. This condition is known as sequestration. Sequestered and extruded fragments may sometimes move up or down in the spinal canal. Very rarely do disc fragments tear the dura and migrate inside the thecal sac. These herniations are known as intradural. 8

What is lumbar stenosis, and how does it develop?
Degeneration does not always lead to a herniated disc. In fact, most of the time, the damaged nucleus slowly wears off without herniation. With time, the joint collapses under body weight. Such gradual loss of physiological disc height leads to spinal stenosis via several mechanisms that should be explicitly explained.
Bulging
As noted above, a healthy nucleus acts like a spring and spreads vertebral bodies apart. This action is necessary to maintain normal disc height. With the weakening of the nucleus due to degeneration, disc height progressively diminishes, resulting in outward bulging of the annulus fibrosus and posterior longitudinal ligament. As a result, the spinal canal narrows.
Ligamentous hypertrophy
With the loss of the nucleus pulpous, the adjacent vertebrae becomes slightly unstable. Therefore, other supporting structures have to be enlarged to restore stability. Ligamentum flavum is one of them, and its hypertrophy is a compensatory mechanism for spinal disc degeneration. Unfortunately, ligamentum flavum hypertrophy causes significant narrowing of the spinal canal.
Loss of intervertebral foraminal height
Degeneration causes disc collapse, which brings vertebral bones closer together. As a result, the height and cross-sectional area of intervertebral foramina drastically decrease, which directly leads to spinal nerve root impingement.
Facet hypertrophy
Under physiological conditions, the facet joints do not take much load (only about 16%). However, with the loss of disc function, they have to compensate and step in. As a result of increased mechanical stress, facet joints suffer and get damaged. The facet bones become larger to hold the weight. Facet hypertrophy further narrows the spinal canal and intervertebral foramina. Hypertrophy of the superior articular process is called “superior facet syndrome.” In this condition, an enlarged superior facet of the lower vertebra causes compression of the exiting nerve root. Another clinical scenario is “lateral recess syndrome.” In this condition, hypertrophic facet bone causes the narrowing of a specific bone gutter known as lateral recess. This gutter contains traversing nerve roots, which get smashed in lateral recess syndrome.
Osteophyte formation
Normally, mechanical load from body weight is evenly distributed through the disc space due to the visco-elastic nature of the healthy nucleus. Disk degeneration causes uneven load distribution and triggers excessive bone growth. Such extra bone protrusions narrow the spinal canal and neural foramina, contributing to stenosis.
Degenerative spondylolisthesis and retrolisthesis
In some cases, disc degeneration causes loss of vertebral alignment. If supporting ligaments and facet joints cannot compensate for loss of stiffness, vertebral bones may lose their normal alignment. Degenerative instability in the affected disc may cause the vertebral bone to slip forward (spondylolisthesis or anterolisthesis) or backward (retrolisthesis). Such misalignments contribute to stenosis and may compress or stretch nerve roots.
Deformity – kyphosis, hyperlordosis and scoliosis
Normally, the lumbar spine has a forward curve, known as lordosis. The spine generally has alternating forward and backward curves, which characterizes a double S-shaped appearance when looking from the side. However, the spine is straight from the front (or back). Severe disc degeneration, particularly at multiple levels, may affect the spine’s shape. It may manifest as loss of lordosis – “flat back syndrome” or lumbar kyphosis, exaggerated lordosis – hyperlordosis, and sometimes loss of coronal balance leading to scoliosis.

What are the symptoms of a lumbar herniated disc?

Low back pain
Lumbar herniated disc symptoms depend on the duration and extent of the process. Degeneration and black disc disease alone trigger low back pain. The mechanical nature of the pain is very specific. Pain is aggravated by load and relieved by resting. Bending forward combined with heavy lifting may trigger an acute low back pain attack. Usually, these attacks last several days to weeks and respond very well to resting and pain medication. Pain might also be aggravated by cold, which is why it is usually worse during winter.
Leg pain and neurological symptoms
The presence of leg pain indicates nerve root compromise and is an early sign of radiculopathy. Usually, this type of pain starts in the lower back region and radiates to the leg. The presence of pain in one extremity is common, yet both legs may be affected. The extent of leg pain depends on the degree of nerve root impingement. Each of the spinal nerves has a specific unique innervation area, and physicians may diagnose the affected nerve root by asking the patient to localize leg pain. Advanced compression compromises nerve function and causes loss of sensation (hypoesthesia) and weakness of the leg muscles (paresis). These symptoms are known as neurological deficits and should alarm patients and physicians. Delays in diagnosis and treatment of neurological deficits usually cause permanent loss of neurological function.
Lumbar stenosis symptoms
Lumbar stenosis causes a specific set of symptoms slightly different from disc herniation. Since the process is very slow, classical radiculopathy is not usually present. Patients often experience “neurogenic claudication,” characterized by the inability to walk long distances without resting. As the disease progresses, walking distances become shorter, significantly compromising the patient’s quality of life. Usually, both legs are involved, though asymmetrical involvement is frequent. Often, patients have some combination of lumbar stenosis and a herniated disc. One should remember that stenosis and herniated discs are the most common scenarios in the natural history of degenerative lumbar disc disease. They frequently co-exist together and may produce mixed symptoms.
Sciatica
Sciatica, characterized by pain radiating along the sciatic nerve down the leg, is one of the common symptoms of lumbar disc herniation. This pain often starts in the lower back and travels through the buttock and down the leg, sometimes reaching the foot. Sciatica symptoms can also include numbness, tingling, and muscle weakness in the affected leg. Physical therapy is often recommended to help alleviate sciatica symptoms.
Diagnosis of lumbar disc herniation
The diagnosis of lumbar disc herniation is made through meticulous clinical examination and radiological assessment. In a typical clinical scenario, clinical examination raises suspicion, and radiological verification confirms the clinical diagnosis and provides information about the extent and stage of the disease.
Once diagnosed, treatment options like physical therapy, epidural injections, or surgery are evaluated based on the severity and progression of the condition, aiming to provide relief and improve the patient’s quality of life.
Clinical Examination
The history of the disease and physical examination are undoubtedly the most crucial parts of the patient’s evaluation. Clinical examination is important for evaluating neurological status and provides crucial information for a correct treatment plan.
History of the disease
Medical history provides valuable clues from the very beginning of communication. One of the most consistent features of degenerative lumbar disease is mechanical low back pain. The pain is either provoked or worsened by mechanical stress like standing, walking, sitting, heavy lifting, or bending forward or backward. Non-mechanical low back pain or chronic back pain should raise suspicion of other diseases. Another typical feature of pain is cold intolerance. However, patients may not mention this detail, among other symptoms, during conversation unless specifically asked.
Paravertebral muscle spasms are a very frequent symptom of degenerative lumbar disease. Patients may specifically indicate that they feel constant “spasticity” or “spasms” in the lower back area.
Leg pain is a sign of nerve root involvement. Slight compression simply irritates the nerve without affecting its function. However, if the patient mentions numbness and weakness, the physician must be alert because it indicates a loss of function.
In many cases, patients already know their diagnosis before visiting doctors. This is a typical situation when patients are referred or have a long history of disease with multiple treatment attempts. Some of them may have prior surgeries.
Neurological Examination
Physical examination of patients with degenerative lumbar spine disease should include neurological examination and several specific tests. Neurological examination is basically focused on looking for sensory and motor deficits. As mentioned above, every spinal nerve root provides innervation to specific skin areas and muscles in the leg. Therefore, a careful neurological examination may reveal which nerve root or roots might be compromised. Of course, the presence and degree of neurological deficit are key factors in formulating the treatment plan. Patients with minimal or no neurological deficits may undergo conservative treatment, while significant or rapidly evolving neurological deficits require prompt surgical intervention.
Lower extremity tension tests
One of the most commonly used tests for a lumbar herniated disc is a straight leg raise (SLR) or Laseque’s test. The patient lies supine during this test, and the examiner passively elevates the leg. If this maneuver induces pain, the test is considered positive. The primary mechanism behind this test is tension on the sciatic nerve and lower lumbar nerve roots. This test has several modifications, including contralateral SLR when pain occurs in the affected leg with unaffected leg elevation. Another variation includes the femoral nerve tensile test, during which the femoral nerve and upper lumbar nerve roots are stretched.
Muscle spasms
Another important part of clinical evaluation is a local examination of the lower back area. Manual palpation or gentle tapping of the affected area may reveal the exact source of the pain. Quite frequently, clinicians encounter paravertebral muscle spasms. These involuntary contractions of back muscles are believed to originate as a response to low back pain and spinal instability and are quite typical for degenerative lumbar spine disease.
Physical examination in lumbar stenosis
Clinical examination of lumbar spinal stenosis patients usually does not reveal much. This is quite striking, given the degree of their complaints. Neurological examination is normal, or near normal, SLR or other tensile tests are negative, and there is minimal or absent tenderness in the lower back area. Such disparity between abundant complaints and fair clinical findings is very typical in spinal stenosis.
Radiological evaluation
Radiological evaluation is an important part of the assessment. Modern radiological tools can precisely diagnose degenerative lumbar disease, making them indispensable for mapping out a treatment plan. Several radiological modalities are used for degenerative spine disease diagnosis, each with its own advantages.
MRI
MRI of the lumbar spine is the diagnostic test of choice. It provides close-up, high-resolution images of the spine in all three planes. MRI sequences (T1, T1, proton density, STIR) can show tissues in different contrasts and provide valuable information.
One of the striking advantages of MRI is the ability to visualize the disc joint and the presence of degeneration directly. In fact, the term “black disc disease” originates from the MRI appearance of the degenerated disc. MRI clearly shows disc degeneration, herniation, and spinal stenosis. Also, it may demonstrate other pathologies like fracture, inflammation, tumor, etc. Nerve root compression is easily identifiable on MRI, as well as the degree and extent of herniation itself. The degree location of concomitant stenosis is also evidently visible on MRI.
X-ray
X-rays provide good information about bones, specifically lumbar spine alignment, presence of deformity, bone spurs, narrowing of the disc spaces, vertebral slippage, etc. They cannot visualize soft tissue, like the disc joint itself or a herniated disc per se. One of the advantages of X-rays is that they can be taken while standing and in various conditions like flexing or extending. Such dynamic evaluation might be useful in some selected cases.
CT scan
CT also utilizes X-rays but with much higher resolution. Like X-ray, it is suitable for bone visualization. CT scans much better demonstrate fractures, misalignments, bone erosions, and osteophytes. It is also possible to reconstruct 3D images from raw scans for better visualization.
EMG and nerve conduction studies
If the diagnosis is doubtful, EMG and nerve conduction studies can be performed in some cases to confirm the presence of radiculopathy. However, their practical usefulness is limited. These studies, however, may help distinguish lumbar radiculopathy from peripheral nerve compression syndromes of the lower extremity.
Next: Lumbar Disc Herniation Treatment
The comprehensive guide on Lumbar Disc Herniation treatment by neurosurgeon Dr Kamran Aghayev: Learn about nonsurgical treatment options like physical therapy and epidural steroid injection for severe pain relief; understand when spine surgery becomes necessary, including surgical treatments such as lumbar discectomy and spinal fusion.
References
- Guerrero J, Hackel S, Croft AS, Hoppe S, Albers CE, Gantenbein B. The nucleus pulposus microenvironment in the intervertebral disc: the fountain of youth? Eur Cell Mater. 2021;41: 707-738. https://doi.org/10.22203/eCM.v041a46[↩][↩]
- Bartels EM, Fairbank JC, Winlove CP, Urban JP. Oxygen and lactate concentrations measured in vivo in the intervertebral discs of patients with scoliosis and back pain. Spine (Phila Pa 1976). 1998;23(1): 1-7; discussion 8. https://doi.org/10.1097/00007632-199801010-00001[↩][↩]
- Inoue N, Orias AAE, Segami K. Biomechanics of the Lumbar Facet Joint. Spine Surg Relat Res. 2020;4(1): 1-7. https://doi.org/10.22603/ssrr.2019-0017[↩]
- Singh K, Masuda K, Thonar EJ, An HS, Cs-Szabo G. Age-related changes in the extracellular matrix of nucleus pulposus and anulus fibrosus of human intervertebral disc. Spine (Phila Pa 1976). 2009;34(1): 10-16. https://doi.org/10.1097/BRS.0b013e31818e5ddd[↩]
- Rajesh N, Moudgil-Joshi J, Kaliaperumal C. Smoking and degenerative spinal disease: A systematic review. Brain Spine. 2022;2: 100916. https://doi.org/10.1016/j.bas.2022.100916[↩]
- Ngo K, Pohl P, Wang D, et al. ADAMTS5 Deficiency Protects Mice From Chronic Tobacco Smoking-induced Intervertebral Disc Degeneration. Spine (Phila Pa 1976). 2017;42(20): 1521-1528. https://doi.org/10.1097/BRS.0000000000002258[↩]
- Bednar DA, Cauda equina syndrome from lumbar disc herniation, CMAJ, 2016, https://doi.org/10.1503%2Fcmaj.150206[↩]
- Choi JY, Lee WS, Sung KH. Intradural lumbar disc herniation–is it predictable preoperatively? A report of two cases. Spine J. 2007;7(1): 111-117. https://doi.org/10.1016/j.spinee.2006.02.025[↩]