What is the cervical disc herniation?
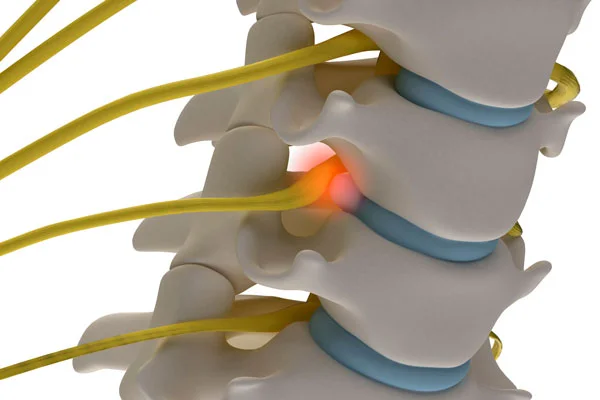
Cervical disc herniation is a condition in which a degenerated intervertebral disc in the neck, also known as the cervical spine, slips into the vertebral canal, causing nerve root and/or spinal cord compression.
Cervical herniated disc signs and symptoms include neck pain, numbness, tingling, weakness in the arms and hands, and, in severe cases, issues with coordination and balance.
What is the structure of the cervical spine?
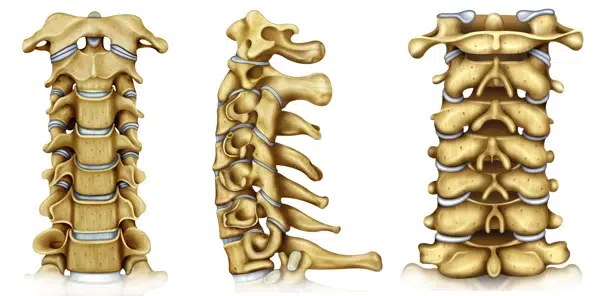
The human head and neck are supported by the cervical spine, a part of the spinal column consisting of seven vertebrae and joints. Each vertebra has a bony arch that forms the spinal canal, which houses and protects the spinal cord. The spinal cord passes through the vertebral canal inside the cervical spine. At each vertebra level, the spinal cord gives off a pair of nerves that pass through the intervertebral foramen to exit the spine. These nerves conduct neural impulses between the spinal cord and the arms.

Each pair of vertebral bones is connected by one large disc joint and two smaller facet joints. The disc joint features a soft, elastic inner core called the nucleus pulposus and a rigid outer ring known as the annulus fibrosus. The nucleus, a unique gel-like substance, acts as an elastic spring between neighboring vertebrae. It provides mobility to the spine and serves as a shock absorber.
A unique feature of the disc joint is the lack of feeding blood vessels. Unlike other bodily organs, intervertebral discs do not have their own blood flow; instead, they extract nutrients and oxygen from adjacent vertebral bones. Therefore, the survival conditions inside the disc are quite harsh. There is very little oxygen and few nutrients available. Only highly specialized chondrocyte-like cells can survive in this environment. Another distinctive feature of the nucleus is its abundance of water and specific types of collagen and proteoglycans. These components give the nucleus its unique mechanical properties.
What is disc degeneration, and how does it lead to cervical disc herniation?
Disc degeneration is a process where the intervertebral discs, which act as cushions between the vertebrae in the spine, gradually deteriorate. Under optimal conditions, cells inside the nucleus remove waste products and replace lost parts, maintaining a delicate balance between wearing out and replacement inside the disc.
However, as with any mechanical component, the disc joint wears out due to mechanical load. At some point in life, the replacement cannot keep up with the wear. As a result, the nucleus pulposus loses water, shrinks, and breaks to pieces. This process is called disc degeneration. It is an irreversible process which has no treatment.
When the nucleus pulposus in the cervical spine degenerates, the disc becomes less flexible and more prone to injury. Fragmented pieces of the degenerated disc can push through the outer layer, the annulus fibrosus, and protrude into the spinal canal. This condition is called cervical disc herniation.
Causes of Cervical Disc Herniation
Cervical spine disc herniation and its underlying condition, cervical disc degeneration, are influenced by various factors that disrupt the physiological balance within the disc. Here are the risk factors and potential causes of herniated discs:
- Age is the most significant risk factor. As individuals age, the mechanisms maintaining disc integrity decline, leading to degeneration.
- Physical inactivity weakens the paraspinal muscles supporting the cervical spine, increasing stress on the discs and accelerating degeneration. Interestingly, a 2021 study from Turkey highlighted advanced disc diseases in young patients, emphasizing that even young, non-sport-oriented individuals are at risk of severe disc herniations. 1
- Genetics: A family history of spine problems increases the risk of early onset and progression of disc degeneration. 2
- Occupation and Lifestyle: Repetitive neck movements, heavy lifting, and poor posture accelerate disc wear and tear. Sedentary lifestyles contribute to poor muscle support and increased spinal load.
- Smoking: Impairs nutrient delivery to disc cells and promotes the breakdown of essential extracellular matrix components. 3
- Obesity: Increases the mechanical load on the cervical spine, accelerating disc degeneration.
- Trauma: Acute or repetitive neck trauma, such as whiplash from car accidents or sports injuries, can initiate or accelerate degeneration.
- Nutritional Factors: Poor diet, dehydration, and conditions impairing nutrient absorption negatively impact disc cell metabolism and repair mechanisms. 4
Complications: what happens if a herniated disc goes untreated?
Cervical herniated disc causes several possible complications if left untreated. The protrusion, or herniation, of the cervical disc can compress the spinal cord and nerve roots, leading to pain, numbness, and weakness in the neck and arms. When a cervical nerve root is compromised, the condition is called cervical spondylotic radiculopathy.
Spinal cord compression is called spondylotic myelopathy. Myelopathy is a more severe condition than radiculopathy and should be promptly treated.
Interestingly, research shows that cervical and thoracic spinal cord compression can also be among the sciatica causes affecting the lower extremities due to similar nerve compression mechanisms. 5
What is cervical stenosis, and how does it develop?
Degeneration does not always result in cervical disc herniation. In fact, most of the time, the damaged nucleus slowly wears off without fragmentation and herniation. In other cases, fragmented parts remain inside the disc joint without herniation. With time, the joint collapses under body weight. Such gradual loss of physiological disc height leads to spinal stenosis via several mechanisms.
Bulging disc
As noted above, a healthy nucleus acts like a spring and spreads vertebral bodies apart. This action is necessary to maintain normal disc height. Degeneration weakens the nucleus, causing the disc height to diminish and the annulus fibrosus and posterior longitudinal ligament to bulge outward. As a result of this bulging, the spinal canal narrows.
Ligamentous hypertrophy
With the loss of the nucleus pulposus, adjacent vertebrae become slightly unstable. To restore stability, other supporting structures, such as the ligamentum flavum, enlarge. This hypertrophy is a compensatory mechanism for disc degeneration. Unfortunately, ligamentum flavum hypertrophy causes significant narrowing of the spinal canal.
Loss of intervertebral foraminal height
Degeneration causes disc collapse, which brings the vertebral bones closer together. As a result, the height and cross-sectional area of the intervertebral foramina drastically decrease, leading to spinal nerve root impingement.
Unco-vertebral joint hypertrophy and deformation
Uncovertebral joints (UVJs), or Luschka’s joints, are paired joints formed by the uncinate processes of the lower vertebra and corresponding joint surfaces of the upper vertebra. These joints flank the disc joint, i.e., the disc joint is located between left and right UVJs. With disc height decrease, the mechanical load on UVJs increases, resulting in hypertrophy, osteophyte formation, and deformity. Cervical spinal nerve roots pass through the intervertebral foramina just posterior and lateral to the UVJs and may get compressed due to hypertrophy.
Extreme hypertrophy may cause Bow Hunter Syndrome due to rotational compression of the vertebral artery passing laterally to the uncinate process, leading to symptoms like dizziness and vertigo. In rare cases, patients may develop a stroke due to a lack of brain blood supply.
Osteophyte (bone spurs) formation
Normally, the mechanical load from body weight is evenly distributed through the disc space due to the visco-elastic nature of the healthy nucleus. Degeneration leads to uneven load distribution and triggers excessive bone growth, known as osteophytes or bone spurs. Such extra bone protrusions may narrow either the spinal canal or neural foramina, contributing to cervical stenosis.
For more information on the effects of spinal osteophytes, you can refer to our article on another degenerative spine condition called DISH disease.
Degenerative spondylolisthesis and retrolisthesis
In some cases, disc degeneration causes a loss of vertebral alignment. If supporting ligaments and facet joints cannot compensate for the loss of stiffness, vertebral bones may lose their normal alignment. Degenerative instability may cause vertebral bones to slip forward (spondylolisthesis or anterolisthesis) or backward (retrolisthesis). Such misalignments contribute to stenosis and may compress or stretch nerve roots.
Kyphosis
Normally, the cervical spine curves forward, which is known as lordosis. The spine generally has alternating forward and backward curves, giving it a characteristic double S-shaped appearance when viewed from the side. Severe disc degeneration, particularly at multiple levels, can affect the spine’s shape. It may manifest as a loss of lordosis or, worse, kyphosis. In extreme cases, the neck may become grossly deformed, resulting in a swan neck deformity.
What are the symptoms of the cervical disc herniation?

Neck pain
Neck pain is the most common symptom of cervical disc herniation. The pain is mechanical, i.e., provoked or worsened by neck movements. Another common feature is cold intolerance. Most patients feel worse during winter and slightly better in summer.
Neuropathic pain, numbness, and weakness (Radiculopathy)
Radiculopathy refers to nerve root compression and manifests as neuropathic pain, numbness (hypoesthesia) and weakness (paresis). Every nerve root provides innervation to specific skin area in the arm as well as certain muscles. Therefore every radiculopathy has unique clinical “signature”. Recognizing this pattern and finding out damaged root is clinician’s duty. Usually, radicular pain and numbness are in the same skin are and therefore numbness may not be appreciated. However, patients are usually well aware of weakness (paresis). In advanced cases, muscle wasting (atrophy) may develop.
Cervical myelopathy symptoms
Cervical spondylotic myelopathy refers to the condition when a degenerated disc causes mechanical compression of the spinal cord. It might be acute or chronic. Typical cervical myelopathy symptoms are numbness, weakness, ataxia (loss of balance), increased reflexes, and urinary incontinence. These symptoms are usually bilateral (present on both sides). Acute myelopathy is usually seen in disc herniations, while the chronic form is typical for cervical canal stenosis. Due to the slow progression of the disease, patients might not be able to relate their symptoms to disc degeneration, especially if the pain is not very severe.
In some cases, progressive atrophy of the spinal cord causes patients to lose pain sensation, further delaying diagnosis. Very frequently, they consider symptoms to be part of normal aging and usually seek medical attention when the herniated disc symptoms are quite severe. Hand muscle atrophy is typical in chronic myelopathy.
Potential Consequences of Chronic Myelopathy
Sometimes features of chronic myelopathy are not very prominent and patients are unaware of them. In these cases relatively minor trauma may have catastrophic consequences. Cervical stenosis significantly decreases spinal cord’s ability to move inside the canal and even a small impact may cause significant injury. The patients may develop very severe neurological symptoms as a consequence of simple trauma.
Bow Hunter Syndrome: Can cervical disc herniation cause dizziness?
In rare cases, bone spurs from cervical disc herniation can lead to a condition known as Bow Hunter Syndrome. This occurs when dynamic rotational compression of the vertebral arteries reduces blood flow to the brain. Symptoms include dizziness, vertigo, and, in severe cases, stroke. Additionally, bone spurs developing in front of the spine can compress the esophagus, leading to swallowing difficulties (dysphagia).
How is the diagnosis of cervical disc herniation made?
The diagnosis of cervical disc herniation is made through thorough clinical examination and radiological evaluation. Both are very important and complement each other. Any discrepancies between clinical and radiological findings should alert the physician and prompt necessary investigation. Failure to do so inevitably results in diagnostic mistakes and treatment fiasco.
Clinical Examination
Proper history and examination are sufficient to suspect the diagnosis. A neurological examination with complete motor and sensory assessment is absolutely necessary since patients might be unaware of their deficits.
History of the disease
History provides valuable clues from the very beginning of communication. One of the most consistent features of degenerative cervical disease is mechanical neck pain.
Arm pain is usually a sign of nerve root and/or spinal cord involvement. Neurological deficits, especially severe ones, point to compression of the vulnerable neural tissue (either roots or spinal cord) and should alert the clinician.
Clinical Examination
Clinical examination of patients with known or suspected degenerative cervical spine disease should include neurological examination and several specific tests. Neurological examination is basically focused on looking for sensory and motor deficits. As mentioned above, every spinal nerve root provides innervation to particular skin areas and muscles in the arm. Therefore, a careful neurological examination may reveal which nerve root is compromised.
Of course, the presence and degree of neurological deficit are key factors in formulating the treatment plan. Patients with minimal or no neurological deficits may undergo conservative treatment, while significant or rapidly evolving neurological deficits require prompt surgical intervention. Atrophy, increased knee-jerk reflexes, and ataxia are almost always associated with myelopathy.
How to test for a herniated disc?
One of the most commonly used tests for cervical disc herniation is Spurling’s test. During this test, a mechanical force is applied to the patient’s head in a tilted position. If pain is induced, the test is positive. The opposite one is the Cervical Distraction test. During this test, the patient’s head is slightly pulled up. If pain decreases or vanishes, the test is positive. Upper Limb Tension Tests (ULTTs) are also used clinically to diagnose cervical disc disease.
Radiological evaluation
Radiological evaluation is a very important part of assessment. Modern radiological tools can precisely diagnose degenerative cervical disease. They are indispensable for mapping out treatment plan. There are several radiological modalities used for the diagnosis of degenerative spine disease. Each modality has its advantages.
MRI

MRI of the cervical spine is the diagnostic test of choice. It gives the best resolution of the spine in all three planes. Multiple magnetic resonance imaging sequences help visualize pathology from various perspectives.
What does a herniated disc look like on an MRI?
One striking advantage of MRI is its ability to visualize the disc joint directly. Degenerated discs appear black on T2W images, unlike healthy white discs. MRI shows herniation, spinal stenosis, and ligamentous hypertrophy. It also helps differentiate other pathologies, such as fracture, inflammation, spinal tumor, etc.
X-ray
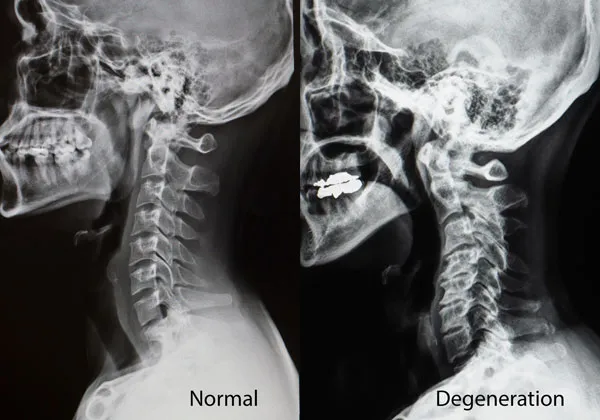
X-rays provide good information about bones, specifically cervical spine alignment, presence of deformity, bone spurs, narrowing of the disc spaces, cervical vertebrae slippage, etc. They cannot visualize soft tissue like the disc joint itself or disc herniation. One of the advantages of X-rays is that they can be taken while standing and in various conditions like flexing or extending. Such dynamic evaluation might be helpful in some selected cases.
CT scan
CT also utilizes X-rays but with much higher resolution. Like X-ray, it is suitable for bone visualization. CT scans much better demonstrate fractures, misalignments, bone erosions, and osteophytes. It is also possible to reconstruct 3D images from raw scans for better visualization.
EMG and nerve conduction studies
In some cases, if the diagnosis is doubtful, EMG, nerve conduction, and evoked potential studies can be performed to confirm the presence of cervical radiculopathy or myelopathy. However, their practical usefulness is limited. These studies help distinguish cervical radiculopathy from peripheral nerve compression syndromes.
Next: Cervical Disc Herniation Treatment
Discover the comprehensive cervical disc herniation treatment guide, including nonsurgical treatments like physical therapy, gentle stretches, and pain management. Learn about cervical disc replacement surgery and cervical discectomy as surgical options to address disc pain and regain mobility, along with insights into the surgery recovery process
References
- Ucar D, Duman S, Bayram Y, Ucar BY, Extruded disc herniations are experienced earlier by inactive young people in the high-tech gaming era, J Med Life, 2021, https://doi.org/10.25122%2Fjml-2021-1059[↩]
- Sambrook P N, MacGregor A J, Spector T D, Genetic influences on cervical and lumbar disc degeneration: a magnetic resonance imaging study in twins, Arthritis Rheum, 1999, https://doi.org/10.1002/1529-0131(199902)42:2%3C366::AID-ANR20%3E3.0.CO;2-6[↩]
- Rajesh N, Moudgil-Joshi J, Kaliaperumal C, Smoking and degenerative spinal disease: A systematic review, Brain Spine, 2022, https://doi.org/10.1016%2Fj.bas.2022.100916[↩]
- Zhu Q, Gao X, Levene HB, Brown MD, Gu W, Influences of Nutrition Supply and Pathways on the Degenerative Patterns in Human Intervertebral Disc, Spine (Phila Pa 1976), 2017, https://doi.org/10.1097%2FBRS.0000000000001292[↩]
- Ito T, Homma T, Uchiyama S, Sciatica caused by cervical and thoracic spinal cord compression, Spine (Phila Pa 1976), 1999, https://doi.org/10.1097/00007632-199906150-00017[↩]