If you’ve been diagnosed with idiopathic intracranial hypertension – sometimes called pseudotumor cerebri – you’ve likely been told your condition has no known cause. That’s what “idiopathic” means in medicine: cause unknown.
You’ve probably been advised to lose weight, take acetazolamide, and hope for the best. If symptoms persist, more invasive options follow: shunts, optic nerve sheath fenestration, venous sinus stents.
But what if “idiopathic” simply means the cause hasn’t been looked for in the right place?
In a meaningful number of patients the cause is mechanical, and it lies outside the brain – in the neck and chest.
What IIH actually is – in plain terms
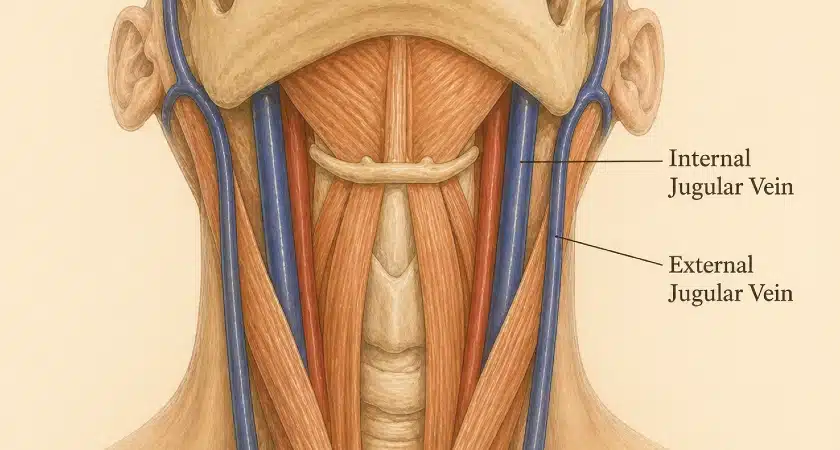
The brain sits in a closed box (the skull) and is surrounded by cerebrospinal fluid (CSF). For pressure inside that box to stay normal, fluid has to be made and drained at matching rates. The drainage isn’t through CSF channels alone – it depends on venous outflow: blood draining from the brain back to the heart through the veins of the neck.
If those veins are obstructed anywhere along their path, pressure backs up: CSF can’t be reabsorbed efficiently, and intracranial pressure climbs. The result is the IIH picture: severe headaches, blurred vision, ringing in the ears (pulsatile tinnitus), and in serious cases, vision loss.
Conventional thinking focuses on what happens inside the skull. The newer understanding – supported by a growing body of imaging and surgical evidence – is that the obstruction is often outside the skull, in the neck and chest.
Two anatomical bottlenecks doctors usually miss
1. The jugular vein at C1
The internal jugular veins are the brain’s main drainage route when you’re lying down. They exit the skull and immediately pass through a narrow corridor between two bony structures: the styloid process of the temporal bone in front, and the transverse process of the C1 vertebra behind.
In some people, that corridor is too narrow. The jugular vein gets pinched between bone and bone – like a garden hose squeezed between two rocks. This is called styloatlantal compression or, in some forms, venous Eagle syndrome.
It’s increasingly recognized as a cause of headaches, brain fog, tinnitus, and intracranial hypertension. Routine imaging often misses it because the vein is only compressed in certain head positions, while standard scans are taken with the head straight.
The clue: headaches that change with head position. They worsen with neck rotation. They’re dramatically affected by sleep position. Patients describe lying flat and waking with crushing pain, sleeping semi-upright by instinct, or tinnitus that disappears when they press on their neck.
2. The thoracic outlet
Lower down, between the collarbone and the first rib, sits another anatomical bottleneck: the thoracic outlet. This is where the subclavian vein passes from the arm into the chest. When this space is too tight, the vein gets compressed in a “nutcracker” between the bone above and the bone below.
The classic version of this is thoracic outlet syndrome (TOS), usually thought of as an arm problem: numbness, tingling, swelling, exertional fatigue. But the consequences can extend upward.
When the subclavian vein is chronically compressed, the body finds alternative routes for blood to drain from the arm. Those alternative routes run through the same veins of the neck that drain the brain – the jugular veins, the vertebral venous plexus (a network of veins running along the spine), and other smaller cervical veins. In a 2014 venographic study by Ahn and colleagues of patients with neurogenic thoracic outlet syndrome, 76% had narrowing of the internal jugular vein – exactly what you would expect when the brain’s drainage pathway is being recruited as a backup for an obstructed arm vein 1
In other words, the brain’s drainage system is now pulling double duty: trying to clear the brain and the arm at the same time. In the standing or sitting position – the posture in which the brain becomes most dependent on these alternative routes – the system can be overwhelmed. The result is impaired cerebral venous outflow and elevated intracranial pressure.
The clue: headaches together with arm symptoms. Numbness, swelling, exertional pain in the upper limb. Headaches that worsen with overhead arm activity or certain arm positions.
Positional headaches: the clinical fingerprint most doctors miss

When the underlying cause of “IIH” is mechanical venous compression, the headache pattern is positional – dramatically affected by body posture and arm position. In a 2025 case series by Cha and colleagues of fifty patients with co-existing chronic migraine and thoracic outlet syndrome, 84% reported headaches that were worse when lying down 2 That kind of recumbent worsening is a mechanical fingerprint, not a migraine feature.
The full pattern usually includes:
- Headache worse on lying down or after sleep, often crushing on waking
- Relieved by sitting or standing up – patients often sleep semi-upright by instinct
- Triggered or worsened by neck rotation
- Pulsatile tinnitus, sometimes one-sided, that may quiet when pressure is applied to the neck
- Brain fog that worsens after head movement
- Co-existing arm or shoulder symptoms – numbness, swelling, exertional fatigue
- Often a personal or family history of joint hypermobility
If two or three of these fit, the standard IIH workup – which usually stops at the skull base – is missing the picture.
Why standard treatments often fail
Most IIH treatments address the consequence of impaired venous outflow rather than the cause:
- Acetazolamide reduces CSF production. Helpful, but doesn’t fix the obstruction.
- CSF shunts divert fluid to relieve pressure – a mechanical bypass, not a cure.
- Optic nerve fenestration protects vision but doesn’t address overall pressure.
- Venous sinus stenting opens narrowed segments of the transverse sinuses (large veins at the back of the brain – the narrowing is called transverse sinus stenosis). But a 2024 systematic review by Lim and colleagues of 694 patients found that 22% had persistent or worsened symptoms after the procedure 3 The stent addresses the downstream finding while leaving the upstream cause untouched.
When the underlying problem is mechanical compression at C1 or at the thoracic outlet, the treatment that actually fixes the disease is surgical decompression of the offending bottleneck. The clinical evidence here goes back forty years. In Raskin’s original 1985 series of thirty TOS patients, thirteen became completely headache-free after first rib resection, and eleven previously disabled patients returned to work 4 Forty years later, the Cha 2025 series cited above documented similar surgical improvements in headache among patients with co-existing TOS and migraine 2 Comparable evidence supports decompression of the jugular vein at C1.
What this means for you
If you have IIH that hasn’t responded to standard treatment, or if your headache pattern includes the clinical fingerprint above – positional worsening, neck-rotation triggers, arm symptoms – it’s worth asking whether your “idiopathic” diagnosis is genuinely without a cause, or simply without one that’s been looked for.
The right diagnosis requires more than a standard MRI. It requires:
- Imaging in the upright posture or with provocative maneuvers (head rotation, arms-up positioning)
- Dynamic venography – imaging that captures the vein in motion, not just at rest
- A clinician who knows where to look – typically a multidisciplinary team that includes neurosurgery, vascular surgery, and neurointervention
Treatment, when the right cause is identified, can be definitive rather than indefinite management.
For the full clinical and scientific case – including the specific imaging findings, the published cohort data, and the references behind the argument – read the in-depth article: How Jugular Vein Compression and Thoracic Outlet Syndrome Drive “Idiopathic” Intracranial Hypertension.
See Also
References
- Ahn SS, Miller TJ, Chen SW, Chen JF. Internal jugular vein stenosis is common in patients presenting with neurogenic thoracic outlet syndrome. Ann Vasc Surg. 2014;28(4):946–950. doi:10.1016/j.avsg.2013.12.009[↩]
- Cha YH, Randall L, Weber J, Ahn S. Treatment of thoracic outlet syndrome to relieve chronic migraine. Clin Anat. 2025;38(3):314–323. doi:10.1002/ca.24242[↩][↩]
- Lim J, Monteiro A, Kuo CC, et al. Stenting for venous sinus stenosis in patients with idiopathic intracranial hypertension: an updated systematic review and meta-analysis of the literature. Neurosurgery. 2024;94(4):648–656. doi:10.1227/neu.0000000000002718[↩]
- Raskin NH, Howard MW, Ehrenfeld WK. Headache as the leading symptom of the thoracic outlet syndrome. Headache. 1985;25(4):208–210. doi:10.1111/j.1526-4610.1985.hed2504208.x[↩]